Urodynamics is a group of tests typically prescribed by a urologists, gynecologist, or urogynecologist that allows them to look at how your lower urinary tract works. Your lower urinary tract includes the urethra (which is the tube that carries urine from your bladder to the outside) and the bladder (which stores urine). This is the only form of testing we have to truly evaluate the function of the lower urinary tract.
Most urodynamic tests focus on the bladder’s ability to hold urine and empty steadily and completely. Urodynamic tests can also show whether the bladder is having involuntary contractions that cause urine leakage.
Urodynamic tests range from simple observation to precise measurements using sophisticated instruments. However, the precise electronic measurement is what is most typically used in modern labs. For precise measurements, advanced electronic equipment and pressure monitors record the pressures inside the bladder, and sensors record muscle and nerve activity. The physician will decide the type of urodynamic test based on the person’s health information, physical exam, and lower urinary tract symptoms (LUTS). The urodynamic test results help diagnose the cause and nature of a lower urinary tract problem. In particular, it is used to properly and fully diagnose the different kinds and causes of incontinence.
Most urodynamics tests do not involve significant preparation, though some tests may require the patient to make a change in fluid intake or to stop taking certain medications. Depending on the test, a person may be instructed to arrive for testing with a full bladder.
If you would offer urodynamics testing in your practice or hospital, click the button below to learn how to provide it with minimum effort and cost.
Urodynamics Procedure Video
This video shows a BHN nurse performing a urodynamics procedure and it includes a thorough explanation urodynamics as well.
Detailed Urodynamics Definition
(for the healthcare professional)
Complete urodynamics testing often include the following:
video urodynamic tests (however this is not always part of a typical procedure)
Each of the above components of a urodynamics test will be explained in more detail below.
Post-void Residual (PVR) Measurement
This urodynamic test measures the amount of urine left in the bladder after urination. The remaining urine is called the post-void residual. Post-void residual can be measured with ultrasound equipment to create a picture of the bladder. Bladder ultrasounds are performed in a healthcare provider’s office, radiology center, or hospital by a specially trained technician and interpreted by a doctor. This is a painless procedure, so anesthesia is not needed. Post-void residual can also be measured using a catheter — a thin flexible tube. A health care provider inserts the catheter through the urethra up into the bladder to remove and measure the amount of remaining urine. A post-void residual of 150 milliliters or more is often a sign that the bladder is not emptying completely.
Catheter measurements are performed in a physician’s office, clinic, or hospital. Local anesthesia may be used. These measurements tend to be mildly uncomfortable but are nothing that a patient should fear.
Uroflowmetry
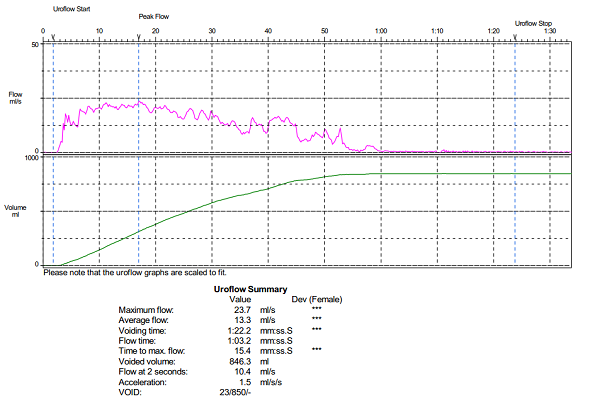
Uroflowmetry is the measurement of urine volume and speed. Special equipment automatically measures the amount of urine and the flow rate — how fast the urine comes out. Uroflowmetry equipment includes a device for collecting and measuring urine and it is attached to a computer that records these measurements. During a uroflowmetry test, the person urinates privately into a special toilet or funnel that has a container for collecting the urine and a scale. The equipment creates a graph that shows changes in flow rate over time so the doctor can see when the flow rate is the highest and how many seconds it takes to get there. Figure 1 below shows an example Uroflometry Chart. Results of this test will be abnormal if the bladder muscles are weak or urine flow is blocked. Another approach to measuring flow rate is to record the time it takes to urinate into a special container that accurately measures the volume of urine. Uroflowmetry measurements are performed in a physician’s office; no anesthesia is needed.
Figure 1 - Uroflowmetry Chart Example
Cystometry - Cystometric Test
A cystometric testmeasures how much pressure builds up inside the bladder as it stores urine, how much urine the bladder can hold, and how full it is when the urge to urinate starts. A catheter, once inserted into the bladder, is used to empty the bladder completely. Then a special, smaller catheter with pressure measuring electrodes is placed in the bladder. This catheter is connected to a pressure-measuring device called a manometer. Another catheter is typically placed in the rectum or vagina to record abdominal pressure. Measuring the difference between the abdominal pressure and the bladder pressure is core to urodynamics.
Once the bladder empties completely, the bladder is filled slowly with warm sterile water using the inserted catheter. During this time, the patient is asked to communicate to the nurse/technician when they feel certain pre-defined bladder sensations. When these pre-defined sensations occur, the volume of water and pressure are recorded. When the urge to urinate occurs, the volume of water and the bladder pressure are recorded. The person may be asked to cough or strain during this procedure to see if there is any urine leakage. A cystometric test can also identify involuntary bladder contractions. Cystometric tests are performed in the physician's office, clinic, or hospital.
Cystometry (or the cystometric test) is in effect recreating the patient's symptoms in a controlled environment with the proper instrumentation in place to gather the diagnostic data coincident with the appearance of each symptom.
Leak Point Pressure Measurement
Leak point pressure (LPP) is the bladder pressure at which involuntary expulsion of urine from the urethral meatus is observed. It is measured while cystometry is being performed. The rise in bladder pressure causing leakage may originate either from the detrusor muscle (caused e.g. by filling a low compliant bladder or by detrusor contractions) or from an increase in abdominal pressure. Thus, there are two different LPP’s, the detrusor leak point pressure and the abdominal leak point pressure — and each is a direct measure of the closure function of the entire bladder outlet under different circumstances.
The detrusor leak point pressure (DLPP) is the value of the detrusor pressure at which leakage occurs in the absence of an abdominal pressure rise. A detrusor leak point pressure > 40 cm H2O is a definite risk factor for urinary tract deterioration, especially if incontinence is an everyday occurrence for the patient. In contrast, the intravesical pressure at leakage during abdominal stress in the absence of a detrusor contraction is called the abdominal leak point pressure. The abdominal pressure increase during the test is obtained voluntarily by coughing (CLPP) or Valsalva. Although higher abdominal presser is reaching during coughing, the Valsalva leak point pressure (VLPP) is better controlled and less variable over time. Often, CLPP is used to test patients who fail to leak on VLPP.
The abdominal leak point pressure is a diagnostic tool for patients with stress incontinence. The leak point pressure is measured by marking on the pressure recording the moment at which urine is expelled from the urethral meatus. This measurement can be made by fluoroscopy, direct visualization, or electric conductance measurements.
Pressure Flow Study
A pressure flow study measures the bladder pressure required to urinate and the flow rate a given pressure generates. After the cystometric test, the person empties the bladder, during which time a manometer is used to measure bladder pressure and flow rate. This pressure flow study helps identify bladder outlet blockage that men may experience with prostate enlargement. Bladder outlet blockage is less common in women but can occur with a cystocele or, rarely, after a surgical procedure for urinary incontinence. Pressure flow studies are performed in a physician’s office, clinic, or hospital. Local anesthesia may be used.
Electromyography
Electromyography, a very common component of urodynamics testing, uses special sensors to measure the electrical activity of the muscles and nerves in and around the bladder and the sphincters. If the physician thinks the urinary problem is related to nerve or muscle damage, electromyography will often be performed. For surface electrode EMG, the sensors are placed on the skin near the rectum. Muscle and nerve activity is recorded electronically using specialized urodynamics equipment. The patterns of the nerve impulses show whether the messages sent to the bladder and sphincters are coordinated correctly. Electromyography is performed by a specially trained technician in a physician’s office or hospital. Anesthesia is not needed.
Video Urodynamic Tests
Video urodynamic tests take pictures and/or videos of the bladder during filling and emptying. The imaging equipment may use x-rays or ultrasound. If x-ray equipment is used, the bladder will be filled with a special contrast fluid, that shows up on x-rays. X-rays are performed by an x-ray technician in a physician’s office, outpatient facility, or hospital. If ultrasound equipment is used, the bladder is filled with warm sterile water and harmless sound waves are used to create a picture of the bladder. The pictures and videos show the size and shape of the bladder and help the health care provider understand the problem. Bladder ultrasounds are performed in the physician's office or hospital by a specially trained technician and interpreted by a doctor, usually a radiologist. Although anesthesia is not needed for the ultrasound, local anesthesia may be used to insert the catheter to fill the bladder.
Video urodynamics is often not part of a typical urodynamics test due to the added expense and because the useful data is derived from the other test components described above.
If you would offer urodynamics testing in your hospital or practice, click the button below to learn how to provide it with minimum effort and cost.